
The hidden epidemic: Physicians who stay but mentally quit
Many physicians stay in their roles but have quietly “quit” in spirit—going through the motions while their passion and engagement vanish.
Many physicians stay in their roles but have quietly “quit” in spirit—going through the motions while their passion and engagement vanish.

Let me confess something that might sound ridiculous coming from a doctor: for most of my career, I treated rest like a threat. A sign of weakness. A guilty pleasure to be earned only after I’d answered every email, seen every patient, signed off every note, and probably rotated the tires on someone else’s car just to be safe.

Is the motive behind resilience training to retain staff so that the system can continue to stay revenue-positive, or is it an investment in the ultimate resource of medicine, the human one?

I am just a physician who has spent 20+ years in the ER, had a few leadership roles along the way (which makes for a mildly robust LinkedIn profile), and nurtured some wisdom too. I think that is enough.

After burning out, I learned that chasing a perfect 50/50 work-life balance is unrealistic—especially in medicine. Instead, I now embrace asymmetric balance, where some days work wins, and others, life does.

Psychological safety, defined as a shared belief that the team is safe for interpersonal risk-taking, is a critical component of effective healthcare delivery. Yet, numerous reports and studies indicate that a lack of psychological safety persists in many healthcare settings, leading to adverse outcomes for both patients and providers.

We humans are wired for connection. Our ancestors evolved as social beings because, simply, working together as a band of humanoids increased their chances of survival and reproduction. Multiple studies have shown that collaboration engenders survival advantage. Yet physician loneliness is a real thing.
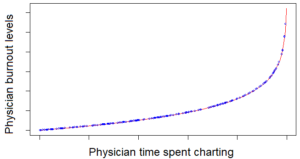
In this article, we look at the connection between charting and physician burnout. We also examine innovations to try and reduce charting-related fatigue and physician burnout.

In this article, we explore the link between the burnout syndrome as it relates to doctors, and the impacts on their physical and mental health.

In this article, we explore the history of the “burnout syndrome” in general and as it relates to physicians specifically. Why is physician burnout history important?

Reach out to your loved ones, and be honest. Trust me, they will help you. You are loved in more ways than you can imagine, because you are one unique lovable bright spot in this world. So stay with us and shine on us. This a Physicians Anonymous co-founder’s story of how she lost a spouse to suicide.

What exactly is physician burnout? In this article, we explore the construct of the burnout syndrome definition as it relates to doctors: a physician burnout definition.
We are not superheroes. We need to navigate the Fine Line Between Appreciation and Realism.

“Front-line”, “battle”, “the trenches”. These terms are all too familiar when talking about modern medicine. Why are we referencing war when we should be talking about healing?
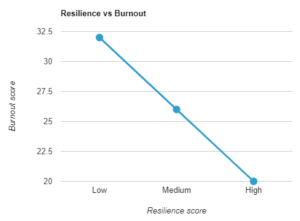
Is there a simple inverse relationship between resilience and burnout? Intuitively, one would think so, but with physicians, it’s never that simple. A recent paper in JAMA Open reveals some startlng findings.

In Part 2, I present the second part of my story: one of physician burnout recovery – how I emerged from the wreckage and rebuilt my life. I sincerely hope that it provides hope for others who are struggling.
If you’ve not heard of Corrigan’s Secret Door, you’re in for a treat. Based on a legendary Irish physician, the Secret Door denotes a metaphorical escape route for busy physicians from their hectic clinics.

My career and life crashed to a halt after 25 years in clinical medicine. I was at one point “suicidal with planning and intent”. Medical knowledge in the hands of a suicidal physician can be deadly. As an affluent, respected physician, confident in my position, well-liked and admired by society, yet suffering inside, why did I not seek help?

In this article, Part 2, I concede that there are some excellent principles differentiating ineffective from effective physician resilience programs. We hope that colleagues and medical leaders designing such programs will find the guidance useful, and further grasp the nettle of addressing the root causes of physician burnout.

Resilience programs, springing up like mushrooms, are a sticking plaster to avoid dealing with the fungating tumor underneath. We have to talk openly about the demands of modern medicine and how these are hurting the healers we need the most.

Practicing medicine is making us physicians sick. Physicians in the US have some of the highest burnout, mental illness, addiction, and suicide rates in the world. Medical student and physician burnout and suicide are a “silent epidemic”.